







The image is potent: a baby with a failing heart, a government-funded device promising salvation and then, cruelly, a budget cut. The narrative writes itself. It indicts the Trump administration, the Department of Government Efficiency (DOGE), and any official with the temerity to ask, “Is this really worth it?” But that very question is not heartless. It is, in fact, the essence of responsible governance.
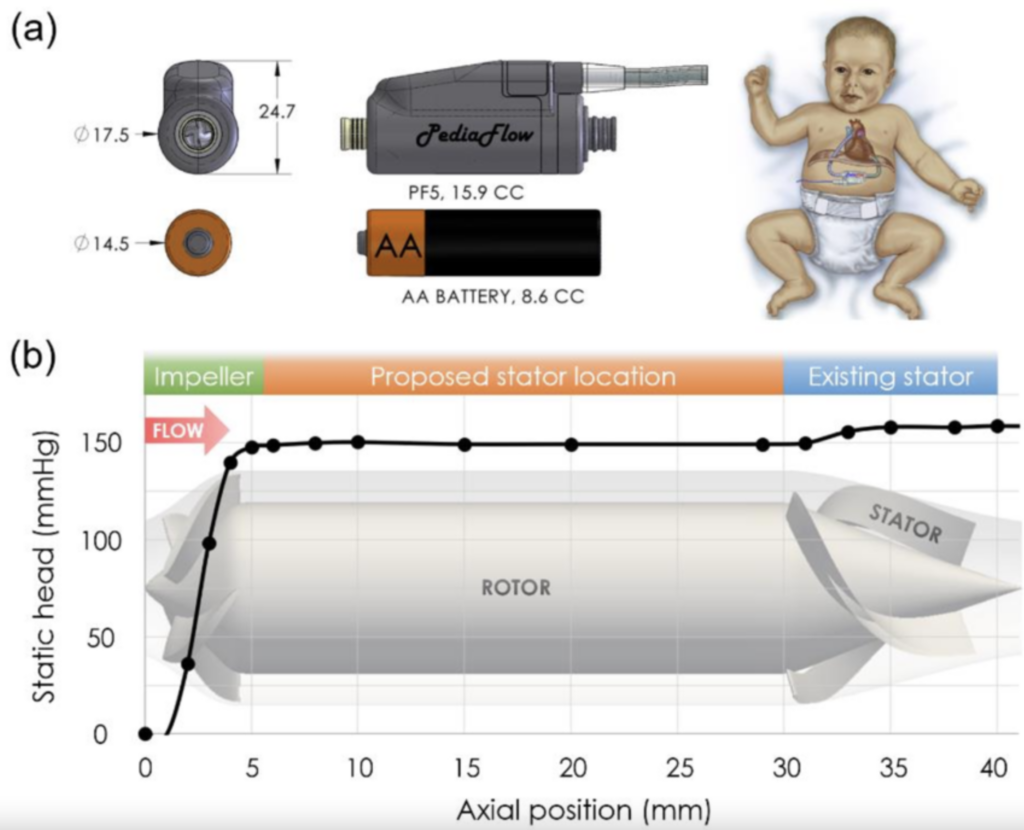
Consider the PediaFlow. A miniature ventricular assist device meant for infants as small as three kilograms, PediaFlow was conceived with noble intent. The project has been shepherded by James Francis Antaki, a distinguished professor at Cornell, who has devoted more than two decades to its development. He is undoubtedly a man of good intentions and scientific insight. Yet good intentions are not sufficient reason to spend taxpayer dollars indefinitely. Especially when what they buy is a promise with no deadline, no viable business model, and no clear path to impact.
Antaki began working on the PediaFlow in 2002. That was 23 years ago. In the time since, Apple has released the iPhone, SpaceX has commercialized rocket launches and a vaccine for COVID-19 was developed in under a year. Meanwhile, PediaFlow remains mired in preclinical stages, dogged by engineering challenges, biocompatibility concerns and theoretical questions about its design. It is difficult to overstate how long two decades is in technological terms. This is not rapid iteration. It is institutionalized stagnation.
The criticisms are not merely procedural or fiscal. They are deeply technical. The PediaFlow design is based on a turbodynamic pump which sacrifices natural hemodynamic pulsatility. In an adult, this is questionable. In an infant, it could be catastrophic. Hemodynamic modeling for this type of device is still underdeveloped, and surrogate indicators for blood clotting risks remain unreliable. Early prototypes failed in predictable ways: clots, power failures, poor flow. That these issues persist two decades into development is not a testament to tenacity, but a red flag of failed execution.
And yet the money flows. In 2019, the Department of Defense awarded Antaki a $4.7 million grant. That money is gone. In March of this year, a new DOD grant of $6.7 million was approved to move the device toward clinical trials. And then, suddenly, it wasn’t. DOGE paused the grant. Not because they oppose the science, or because they are hostile to sick children, but because they are doing what no one has done before: asking for accountability. And here’s a question that no one in the media seems brave, or informed, enough to ask: why is the Department of Defense funding research on infant heart implants in the first place? Is the Pentagon qualified to fund pediatric research much less medical device development? Is it even remotely qualified to award or oversee these kinds of grants? Or has the military budget simply become a bloated slush fund, doling out billions to science projects that have little to no connection to national security?
The outrage from the media was immediate and predictable. Trump is killing babies, they said. The cut will cost lives, they wailed. The narrative is easy to sell: a photo of a NICU, a grieving parent, a supposed miracle withheld by heartless bureaucrats. But behind the emotive veneer is a simple economic reality: the United States is out of money.
We are not spending tax revenue. We are spending borrowed money. We are spending our grandchildren’s prosperity. Every million dollars allocated to an unproven pediatric device is a million not spent educating our children, securing the border, upgrading air traffic control or keeping our defense industrial base solvent. And unlike charity, which depends on the conviction of private donors, government funding is coerced. It is taken by force from millions who have no say in whether they would support this particular longshot.
Let us be honest. PediaFlow is not close to market. Even in the best case, it will require another $20 million and six more years to reach commercialization. That is if everything goes right. And it might not. After 23 years, that is not a pessimistic scenario. It is a conservative estimate. What are we buying with this investment? Possibly a few dozen lives per year, once the device becomes available. Each one, precious. But is that a scalable solution? Is that a viable investment? Or is it the most inefficient way imaginable to achieve a moral good?
Suppose you were to treat this like a business. Let us say you eventually sell 200 units per year, each at $1,000. That yields $200,000 in annual revenue. At that rate, the $27 million investment can never be repaid, even before considering manufacturing costs, liability insurance, or the cost of regulatory compliance. From a purely financial standpoint, this is insolvent from the start. And that, more than anything, is the point.
Science is not immune to scrutiny simply because it wears a lab coat. The fact that someone calls a project “research” does not mean it deserves eternal funding. There must be exit criteria, milestones, deliverables. Without these, grants become pensions. They fund people, not progress.
To be clear: no one is suggesting that projects like PediaFlow should not exist. Rather, we are suggesting that they should not be funded by a government that is hemorrhaging cash. Private donors can fund this work. Corporate sponsors, philanthropic trusts or crowdfunding campaigns can support it if the need is so urgent. And if those avenues fail, that tells us something too: perhaps the project, for all its noble aims, does not inspire confidence.
This is not cruelty. It is prudence. It is the job of the president and his administration to steward the public purse, not to chase every heart-tugging headline. DOGE exists to find exactly this kind of inefficiency. The goal is not to humiliate scientists or deny hope to sick children. The goal is to enforce a standard of evidence and efficiency that should have existed all along.
And let us not forget: the number of children who die annually from congenital heart defects is not 40,000, as some headlines imply. It is between 100 and 200. This is not to minimize the loss. Each child matters. But the scale matters too. Is $27 million for a speculative fix to a problem affecting 200 families a year the best use of limited funds? Or are there more efficient ways to reduce childhood mortality?
The left does not want this conversation. They prefer emotion to arithmetic. They believe that citing “the babies” is sufficient to end debate. It is not. The true measure of compassion is not how loudly one protests, but how wisely one allocates. The Trump administration is not cutting pediatric research to be cruel. It is cutting projects that no longer make sense, that have failed to deliver, that need to be reconsidered. That is not a war on science. It is a war on bad investment.
Perhaps Professor Antaki will find other sponsors. Perhaps he will prove the skeptics wrong and bring the PediaFlow to market. If so, good. Let him be praised. But it should not be on the back of American taxpayers who are already underwriting more debt than at any time in history.
We are long past the point where good intentions are enough. Results matter. Timelines matter. Accountability matters. If we are to save our country from fiscal collapse, we must learn to say no even when it hurts. Especially when it hurts.
Sponsored by the John Milton Freedom Foundation, a nonprofit dedicated to helping independent journalists overcome formidable challenges in today’s media landscape and bring crucial stories to you.
READ NEXT: Revealed: Who’s Continuing To Silence Dissent Online And How






















Oooooo
You said, “All babies lives matter”!
There goes the intersections!
The other side has a war on babies.